Error processing SSI file

2010-2011 Influenza Season Week 51 ending December 25, 2010
All data are preliminary and may change as more reports are received.
Synopsis:
During week 51 (December 19-25, 2010), influenza activity in the United States continued to increase.
- Of the 3,284 specimens tested by U.S. World Health Organization (WHO) and National Respiratory and Enteric Virus Surveillance System (NREVSS) collaborating laboratories and reported to CDC/Influenza Division, 689 (21.0%) were positive for influenza.
- The proportion of deaths attributed to pneumonia and influenza (P&I) was at the epidemic threshold.
- One influenza-associated pediatric death was reported and was associated with Influenza A (H3) virus infection.
- The proportion of outpatient visits for influenza-like illness (ILI) was 2.7%, which is above the national baseline of 2.5%. Two of the 10 regions (Regions 2 and 4) reported ILI above region-specific baseline levels; three states and New York City experienced high ILI activity, six states experienced moderate ILI activity, five states experienced low ILI activity, 35 states experienced minimal ILI activity, and data were insufficient from the District of Columbia and two states.
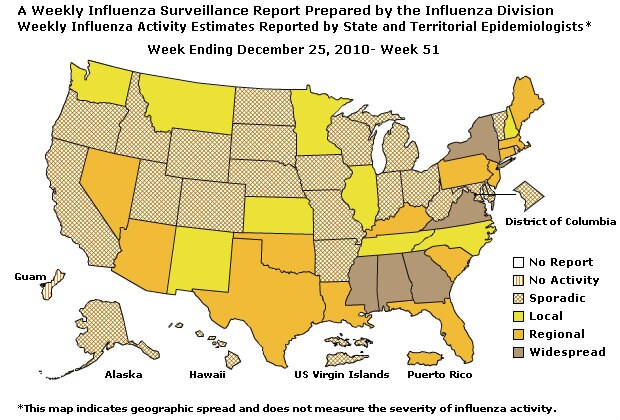
- The geographic spread of influenza in five states was reported as widespread, Puerto Rico and 13 states reported regional activity; nine states reported local activity; the District of Columbia, the U.S. Virgin Islands, and 23 states reported sporadic activity, and Guam reported no activity.
| HHS Surveillance Regions* | Data for current week | Data cumulative since October 3, 2010 (Week 40) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Out-patient ILI† | % positive for flu‡ | Number of jurisdictions reporting regional or widespread activity§ | A (H3) | 2009 A (H1N1) | A(Subtyping not performed) | B | Pediatric Deaths | |||
| Nation | Normal | 21.0% | 18 of 54 | 1,334 | 228 | 1,341 | 1,961 | 3 | ||
| Region 1 | Normal | 18.6% | 3 of 6 | 108 | 7 | 0 | 5 | 0 | ||
| Region 2 | Elevated | 10.4% | 3 of 4 | 77 | 5 | 101 | 10 | 2 | ||
| Region 3 | Normal | 10.6% | 2 of 6 | 122 | 38 | 12 | 19 | 0 | ||
| Region 4 | Elevated | 23.4% | 6 of 8 | 266 | 75 | 776 | 1,547 | 0 | ||
| Region 5 | Normal | 14.6% | 0 of 6 | 138 | 20 | 12 | 31 | 0 | ||
| Region 6 | Normal | 18.8% | 3 of 5 | 139 | 7 | 197 | 136 | 1 | ||
| Region 7 | Normal | 8.8% | 0 of 4 | 24 | 5 | 48 | 18 | 0 | ||
| Region 8 | Normal | 16.8% | 0 of 6 | 334 | 39 | 158 | 21 | 0 | ||
| Region 9 | Normal | 8.8% | 2 of 5 | 94 | 31 | 30 | 167 | 0 | ||
| Region 10 | Normal | 2.8% | 0 of 4 | 32 | 1 | 7 | 7 | 0 | ||
*HHS regions (Region 1 CT, ME, MA, NH, RI, VT; Region 2: NJ, NY, Puerto Rico, US Virgin Islands; Region 3: DE, DC, MD, PA, VA, WV; Region 4: AL, FL, GA, KY, MS, NC, SC, TN; Region 5: IL, IN, MI, MN, OH, WI; Region 6: AR, LA, NM, OK, TX; Region 7: IA, KS, MO, NE; Region 8: CO, MT, ND, SD, UT, WY; Region 9: AZ, CA, Guam, HI, NV; and Region 10: AK, ID, OR, WA).
† Elevated means the % of visits for ILI is at or above the national or region-specific baseline
‡ National data are for current week; regional data are for the most recent three weeks
§ Includes all 50 states, the District of Columbia, Guam, Puerto Rico, and U.S. Virgin Islands
U.S. Virologic Surveillance:
WHO and NREVSS collaborating laboratories located in all 50 states and Washington D.C. report to CDC the number of respiratory specimens tested for influenza and the number positive by influenza type and subtype. The results of tests performed during the current week are summarized in the table below.
| Week 51 | |
|---|---|
| No. of specimens tested | 3,284 |
| No. of positive specimens (%) | 689 (21.0%) |
| Positive specimens by type/subtype | |
| Influenza A | 479 (69.5%) |
| A (2009 H1N1) | 15 (3.1%) |
| A (subtyping not performed) | 277 (57.8%) |
| A (H3) | 187 (39.0%) |
| Influenza B | 210 (30.5%) |
The District of Columbia and 48 states from all 10 surveillance regions have reported laboratory-confirmed influenza this season. While activity in other areas of the country is increasing, Region 4 in the Southeastern United States has accounted for 2,664 (54.8%) of all 4,864 reported influenza viruses this season, including 1,547 (78.9%) of the 1,961 influenza B viruses.
View WHO-NREVSS Regional Bar Charts | View Chart Data | View Full Screen | View PowerPoint Presentation
Aggregate Hospitalization and Death Reporting Activity (AHDRA):
This system tracks weekly counts of laboratory-confirmed influenza-associated hospitalizations and deaths and was implemented on August 30, 2009, during the 2009 pandemic, and ended on April 4, 2010. AHDRA surveillance during the 2010-11 season is being continued on a voluntary basis and 19 jurisdictions reported during week 51. From October 3-December 25, 2010, 961 laboratory-confirmed influenza associated hospitalizations and 19 laboratory-confirmed influenza associated deaths were reported to CDC.
View Full Screen | View Chart Data | View PowerPoint Presentation
Antigenic Characterization:
CDC has antigenically characterized 117 influenza viruses [13 2009 influenza A (H1N1) viruses, 54 influenza A (H3N2) viruses, and 50 influenza B viruses] collected by U.S. laboratories since October 1, 2010.
- All 13 were characterized as A/California/7/2009-like, the influenza A (H1N1) component of the 2010-11 influenza vaccine for the Northern Hemisphere.
2009 Influenza A (H1N1) [13]
- All 54 were characterized as A/Perth/16/2009-like, the influenza A (H3N2) component of the 2010-11 influenza vaccine for the Northern Hemisphere.
Influenza A (H3N2) [54]
- All 50 viruses belong to the B/Victoria lineage of viruses and was characterized as B/Brisbane/60/2008-like, the recommended influenza B component for the 2010-11 Northern Hemisphere influenza vaccine.
Influenza B [50]
Antiviral Resistance:
Testing of 2009 influenza A (H1N1), influenza A (H3N2), and influenza B virus isolates for resistance to neuraminidase inhibitors (oseltamivir and zanamivir) is performed at CDC using a functional assay. Additional 2009 influenza A (H1N1) clinical samples are tested for a single known mutation in the neuraminidase protein of the virus that confers oseltamivir resistance (H275Y). The data summarized below combine the results of both test methods and includes samples that were tested as part of routine surveillance purposes; it does not include diagnostic testing specifically done because of clinical suspicion of antiviral resistance.
High levels of resistance to the adamantanes (amantadine and rimantadine) persist among 2009 influenza A (H1N1) and A (H3N2) viruses (the adamantanes are not effective against influenza B viruses) circulating globally. As a result of the sustained high levels of resistance, data from adamantane resistance testing are not presented weekly in the table below.
| Samples tested (n) | Resistant Viruses, Number (%) | Samples tested (n) | Resistant Viruses, Number (%) | |
|---|---|---|---|---|
| Oseltamivir | Zanamivir | |||
| Seasonal Influenza A (H1N1) | 0 | 0 (0.0) | 0 | 0 (0.0) |
| Influenza A (H3N2) | 33 | 0 (0.0) | 33 | 0 (0.0) |
| Influenza B | 54 | 0 (0.0) | 54 | 0 (0.0) |
| 2009 Influenza A (H1N1) | 17 | 0 (0.0) | 15 | 0 (0.0) |
To prevent the spread of antiviral resistant virus strains, CDC reminds clinicians and the public of the need to continue hand and cough hygiene measures for the duration of any symptoms of influenza, even while taking antiviral medications. Additional information on antiviral recommendations for treatment and chemoprophylaxis of influenza virus infection is available at http://www.cy118119.com/flu/antivirals/index.htm.
Pneumonia and Influenza (P&I) Mortality Surveillance
During week 51, 7.5% of all deaths reported through the 122-Cities Mortality Reporting System were due to P&I. This percentage was at the epidemic threshold of 7.5% for week 51.
View Full Screen | View PowerPoint Presentation
Influenza-Associated Pediatric Mortality
One influenza-associated pediatric death was reported to CDC during week 51 (New York City). This death was associated with an influenza A (H3) virus infection. The death reported this week occurred between December 5, 2010 and December 11, 2010.
Three influenza-associated pediatric deaths occurring during the 2010-2011 season have been reported; two deaths were associated with influenza A (H3) virus infection and one was associated with an influenza A virus for which the subtype was not determined.
View Full Screen | View PowerPoint Presentation
Influenza-Associated Hospitalizations
The Influenza Hospitalization Network (FluSurv-NET) conducts surveillance for population-based, laboratory-confirmed influenza-related hospitalizations in children (persons younger than 18 years) and adults. The network covers over 80 counties in the 10 Emerging Infections Program (EIP) states (CA, CO, CT, GA, MD, MN, NM, NY, OR, and TN) and six additional states (ID, MI, OH, OK, RI and UT). FluSurv-NET estimated hospitalization rates will be updated every two weeks starting later this season.
Outpatient Illness Surveillance:
Nationwide during week 51, 2.7% of patient visits reported through the U.S. Outpatient Influenza-like Illness Surveillance Network (ILINet) were due to influenza-like illness (ILI). This percentage is above the national baseline of 2.5%.
The increase in the percentage of patient visits for ILI may be influenced in part by a reduction in routine healthcare visits during the holiday season, as has occurred in previous seasons.
View ILINet Regional Charts | View Chart Data | View Full Screen | View PowerPoint Presentation
On a regional level, the percentage of outpatient visits for ILI ranged from 0.4% to 4.8% during week 51. Two of the 10 regions (Regions 2 and 4) reported a proportion of outpatient visits for ILI above their region-specific baseline levels.
ILINet State Activity Indicator Map:
Data collected in ILINet are used to produce a measure of ILI activity* by state. Activity levels are based on the percent of outpatient visits in a state due to ILI and are compared to the average percent of ILI visits that occur during spring and fall weeks with little or no influenza virus circulation. Activity levels range from minimal, which would correspond to ILI activity from outpatient clinics being below the average, to high, which would correspond to ILI activity from outpatient clinics being much higher than the average. Because the clinical definition of ILI is very general, not all ILI is caused by influenza; however, when combined with laboratory data, the information on ILI activity provides a clear picture of influenza activity in the United States.
During week 51, the following ILI activity levels were experienced:
- New York City and three states (Alabama, Georgia, and Mississippi) experienced high ILI activity.
- Six states (Arizona, Florida, Illinois, Kentucky, Louisiana, and Nevada) experienced moderate ILI activity.
- Five states (Idaho, Oklahoma, Tennessee, Texas, and Virginia) experienced low ILI activity.
- Minimal ILI activity was experienced by 35 states (Alaska, California, Colorado, Connecticut, Delaware, Hawaii, Indiana, Iowa, Kansas, Maine, Maryland, Massachusetts, Michigan, Minnesota, Missouri, Montana, Nebraska, New Hampshire, New Jersey, New Mexico, New York, North Carolina, North Dakota, Ohio, Oregon, Pennsylvania, Rhode Island, South Carolina, South Dakota, Utah, Vermont, Washington, West Virginia, Wisconsin, and Wyoming).
- Data were insufficient to calculate and ILI activity level from the District of Columbia and one state (Arkansas).
*This map uses the proportion of outpatient visits to health care providers for influenza-like illness to measure the ILI activity level within a state. It does not, however, measure the extent of geographic spread of flu within a state. Therefore, outbreaks occurring in a single city could cause the state to display high activity levels.
Data collected in ILINet may disproportionately represent certain populations within a state, and therefore, may not accurately depict the full picture of influenza activity for the whole state.
Data displayed in this map are based on data collected in ILINet, whereas the State and Territorial flu activity map are based on reports from state and territorial epidemiologists. The data presented in this map is preliminary and may change as more data is received.
Differences in the data presented by CDC and state health departments likely represent differing levels of data completeness with data presented by the state likely being the more complete.
Geographic Spread of Influenza as Assessed by State and Territorial Epidemiologists:
The influenza activity reported by state and territorial epidemiologists indicates geographic spread of influenza viruses, but does not measure the severity of influenza activity.
During week 51, the following influenza activity was reported:
- Widespread influenza activity was reported by five states (Alabama, Georgia, Mississippi, New York, and Virginia).
- Regional influenza activity was reported by Puerto Rico and 13 states (Arizona, Connecticut, Florida, Kentucky, Louisiana, Maine, Massachusetts, Nevada, New Jersey, Oklahoma, Pennsylvania, South Carolina, and Texas).
- Local influenza activity was reported by nine states (Illinois, Kansas, Minnesota, Montana, New Hampshire, New Mexico, North Carolina, Tennessee, and Washington).
- Sporadic influenza activity was reported by the District of Columbia, the U.S. Virgin Islands, and 23 states (Alaska, Arkansas, California, Colorado, Delaware, Hawaii, Idaho, Indiana, Iowa, Maryland, Michigan, Missouri, Nebraska, North Dakota, Ohio, Oregon, Rhode Island, South Dakota, Utah, Vermont, West Virginia, Wisconsin, and Wyoming).).
- Guam reported no influenza activity.
- Content Source: Coordinating Center for Infectious Diseases (CCID)
- National Center for Immunization and Respiratory Diseases (NCIRD)
Additional National and International Influenza Surveillance Information
U.S. State and local influenza surveillance: Click on a jurisdiction below to access the latest local influenza information.
Distribute Project: Additional information on the Distribute syndromic surveillance project, developed and piloted by the International Society for Disease Surveillance (ISDS) now working in collaboration with CDC, to enhance and support Emergency Department (ED) surveillance, is available at http://isdsdistribute.org/
Google Flu Trends: Google Flu Trends uses aggregated Google search data in a model created in collaboration with CDC to estimate influenza activity in the U.S. For more information and activity estimates from the U.S. and worldwide, see http://www.google.org/flutrends/
Europe: for the most recent influenza surveillance information from Europe, please see WHO/Europe at http://www.euroflu.org/index.php and visit the European Centre for Disease Prevention and Control at http://ecdc.europa.eu/en/Activities/Surveillance/EISN/Pages/home.aspx
Public Health Agency of Canada: The most up to date influenza information from Canada is available at http://www.phac-aspc.gc.ca/fluwatch/
World Health Organization FluNet: Additional influenza surveillance information from participating WHO member nations is available at http://gamapserver.who.int/GlobalAtlas/home.asp
--------------------------------------------------------------------------------
A description of surveillance methods is available at: http://www.cy118119.com/flu/weekly/overview.htm
